
Anorexia nervosa (AN) is a well-recognized eating disorder characterized by “restriction of energy intake relative to requirements” (American Psychiatric Association 2013). Sometimes regarded as a physiological disorder—we are easily able to generate a mental image of the emaciated anorexic physique—the current Diagnostic and Statistical Manual of Mental Disorders (DSM-5) emphasizes the psychological disturbance that leads to emaciation, including in its diagnostic criteria an “intense fear of gaining weight … or behavior that interferes with weight gain” (American Psychiatric Association 2013). In fact, the DSM-5 goes so far as to require resolution of this disturbance for an anorexic to achieve complete remission. Clinical awareness of AN’s status as a mental disorder has made it such that, excepting severe cases in which malnutrition has compromised organ function, treatment approaches to AN tend to directly address the cognitive and affective aspects of the illness, with the hope that a reduction in the patient’s disordered patterns of thinking will translate to a reduction in the patient’s disordered patterns of behavior. One such approach is cognitive behavioral therapy (CBT). In AN-directed CBT, the clinician encourages the anorexic to interact critically with their valuation of weight and shape, posing questions such as “Is it functional for you to conform to this idea?” or “What role will your present concerns about weight play in your life five years from now?” (Garner and Bemis 1982). Given the success of CBT in ultimately disrupting disordered behavior—a 2017 trial of eating-behavior-focused CBT produced remission and relapse rates of 75% and 10%, respectively (Södersten et al. 2017)—it’s important to similarly consider outcomes among anorexics who refuse to participate in treatment. What effect does a formal diagnosis of AN have on the behavior of those who decide not to pursue treatment? Some intra- and inter-personal factors are common to anorexics and probably support the view that, in the absence of treatment, a diagnosis serves to exacerbate existing disorder-related behavioral symptoms: (1) competition; (2) lack of motivation to challenge anorexic behavior; (3) the ego-syntonic nature of AN.
Factor 1: Competition
Often unspoken, competition seems to be fierce among anorexics. In Anorexia and Mimetic Desire, social philosopher Rene Girard explains that much of anorexic behavior can be understood in terms of mimesis, or imitation. The characteristic drive for thinness of AN, argues Girard, is a consequence of mimetic desire. Or, “we principally experience desire based on seeing other people desire something, rather than on some intrinsic value of the desired object itself” (Strand 2018). Applied to AN, the pervasiveness of a thin ideal—thinness is the object of desire—creates an intense rivalry between sufferers of AN, exacerbating disordered behavior. Each anorexic strives to achieve a ‘better’ thinness than the other, with the ‘best’ thinness being that which causes fainting spells, organ failure, and culminates in death. Allegedly, this exact kind of mimesis has occurred since the 19th century: “At some encounter of their two imperial husbands, [Empress Eugenie of France and Empress Elizabeth of Austria] retired to a private room for the purpose of … comparing their respective waistlines” (Girard 2008).
This sense of inter-personal competition, which already exists in the undiagnosed anorexic, will almost certainly be heightened by a formal diagnosis of AN. Whereas the pre-diagnosis anorexic is on the outside looking in, the post-diagnosis anorexic gains a sort of formal status as a member of the anorexic in-group, and competes at an elite, clinically-recognized level of the illness. Nowhere is this made more apparent than across the various internet forums dedicated to promoting eating disorders. Referred to as ‘pro-anorexia’ or ‘pro-ana’ sites, these online communities allow sufferers of a relatively uncommon illness—irrespective of gender, lifetime prevalence of AN is below 5% (van Eeden et al. 2007)—to commiserate and, much like Eugenie and Elizabeth, to encourage the progression of others’ disordered behavior. A kind-of-disturbing-but-unsurprising thread on Eating Disorder Central created by a user seeking advice on appetite suppression features replies illustrating this morbid egging-on: “Try some natural stimulants to kill your appetite, personally I have to … recommend rauwolscine … it’s a wonder powder! But it will make you feel like you just hit a crack pipe” (Eating Disorder Central 2023).
Factor 2: Lack of motivation to challenge anorexic behavior
There’s a well-established link between persistence of disordered behavior and willingness to engage with a program of treatment: “Higher baseline motivation across … measures [on the Anorexia Nervosa Stages of Change Questionnaire] predicted significant decreases in eating pathology” (Wade et al. 2009). Even though demographic considerations are important in forecasting receptivity or resistance to treatment—as an example, male anorexics tend to be admitted to inpatient programs at a later age than their female counterparts (Gueguen et al. 2012)—the contribution of motivation to both participation in treatment and any subsequent reduction in disordered behavior across all anorexics shouldn’t be discounted. With this in mind, it makes sense to predict that, following diagnosis, an anorexic who declines the clinician’s offer for treatment may do so because they lack the motivation to modify current behavioral patterns, preventing a treatment-facilitated reduction in these behavioral patterns. I think that a refusal to reduce disordered behavior is a tacit agreement to exacerbate disordered behavior.
Factor 3: Ego-syntonic nature of AN
Ego-syntonicity, a concept introduced by Freud, describes illness features that are “valued by those who suffer from [the illness]” (Gregertsen et al. 2017). The ego-syntonic phenomenon in AN is captured by qualitative research: a 2006 study of AN in adolescent patients revealed that restriction-associated weight loss precipitates “a sense of mastery and self-control,” and that the alarm caused by conspicuous emaciation “allows the person with AN to experience the attentiveness, thoughtfulness … and kindness which they may have previously craved” (Freedman et al. 2006). I’d say these findings could underline a lack of motivation to engage with treatment, since participation in even a short outpatient program of CBT would ask the anorexic to part ways with the behaviors that have formed their self-concept.
Going a little further, these findings help justify the claim that a post-diagnosis refusal of treatment is likely to lead to exacerbated disordered behavior. As one of the diagnostic criteria for moderate AN, the patient’s BMI must not exceed 16.99 kg/m2. Having established that a low body weight is valued due to AN ego-syntonicity, a formal diagnosis of moderate AN might very well serve as confirmation to the anorexic that their efforts to practice “self-control” have been recognized. Why should the anorexic stop what they’re doing? Why should they agree to be admitted to an inpatient program in which they’ll be forced (yes, forced) to gain weight and reverse their highly-prized progress? It seems these are the questions that anorexics ask themselves: in the United States, just about one-third of those diagnosed with AN undergo illness-specific treatment (National Institute of Mental Health).
Potential assessment
Right now, I’m thinking back to a one-semester experimental design class I took in college (shoutout to Dr. Smith and Behavioral Assessment of Animal Models of Cognition and Neuropsychiatric Disorders). If we want to determine whether a formal diagnosis of AN leads to exacerbated behavioral pathology, we should evaluate pathology both before and after the diagnosis is made. One useful measure of AN-specific disordered behavior is the restraint subscale of the Eating Disorder Examination Questionnaire (EDE-Q). The EDE-Q is recognized as a standard self-report diagnostic tool for a range of eating disorders, and specifically assess behaviors and attitudes across four subscales: restraint, eating concern, shape concern, and weight concern.
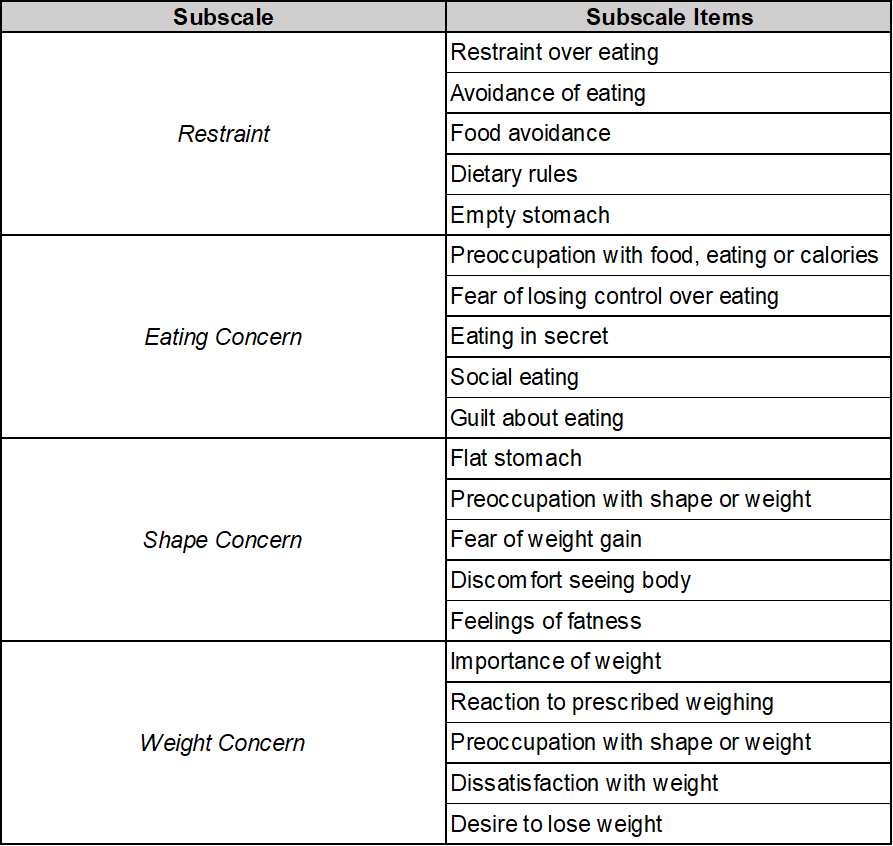
Adapted from Eating Disorder Examination, edition 17.0D
In evaluating the potential impact of a formal AN diagnosis on anorexic behavior, comparisons of restraint subscale scores on the EDE-Q at the time of diagnosis and six months following diagnosis could be made; restraint subscale scores are most relevant because the restraint subscale items describe active disordered behaviors involved in AN ego-syntonicity, like restriction of overall intake and avoidance of specific foods. If a diagnosis of AN really does worsen disorder-related behavioral symptoms in the context of treatment refusal, the expectation would be for six-month scores to indicate more severe restrictive symptoms relative to at-time-of-diagnosis scores for anorexics who reject treatment.
